Ovarian Cancer: Types, Risk Factors, Prevention, Symptoms, Signs, Diagnosis and Prognosis
Overview of the Ovarian Cancers
Overview of the Ovarian Cancers
In general, the term “ovarian cancer” is often used to describe cancers that begin in the cells in the ovary. The cancers are closely related and are generally treated the same way. When the term “ovarian cancer” is used, it includes both fallopian tube and peritoneal cancers, because it may be unclear where cancer started.
These types of cancer begin when healthy cells in these areas change and grow out of control, forming a mass called a tumor. A tumor can be cancerous or benign. A cancerous tumor is malignant, meaning it can grow and spread to other parts of the body. A benign tumor means the tumor can grow but will not spread.
An ovarian cyst is an abnormal growth of tissue that forms on the surface of the ovary. It can occur during a woman’s normal menstrual cycle and usually goes away without treatment. Simple ovarian cysts are not cancerous.
Recent research studies suggest that most ovarian/fallopian tube cancers are high-grade serous cancers (HGSC), and in most cases, cancer actually starts in the distal, or outer, end of the fallopian tubes. Then, it spreads to the surface of the ovaries and beyond.
Based on this new knowledge, some doctors recommend the removal of the fallopian tubes rather than tying or banding the tubes for contraception (to avoid future pregnancy).
Some doctors also recommend fallopian tube removal when a woman is undergoing surgery for benign disease and does not want to get pregnant in the future. This strategy could prevent the development of these cancers in the future. Talk with your doctor about whether this may be an option for you.
Because the surfaces of the ovaries, the lining of the fallopian tubes, and the covering cells of the peritoneum are made up of the same types of cells, most of these diseases look alike under a microscope.
Overview of the Ovaries
The ovaries are part of a woman’s reproductive system. There are 2 ovaries, with 1 located on each side of the uterus. In premenopausal women, they are almond-shaped and about 1.5 inches long. These glands contain germ cells, also called eggs.
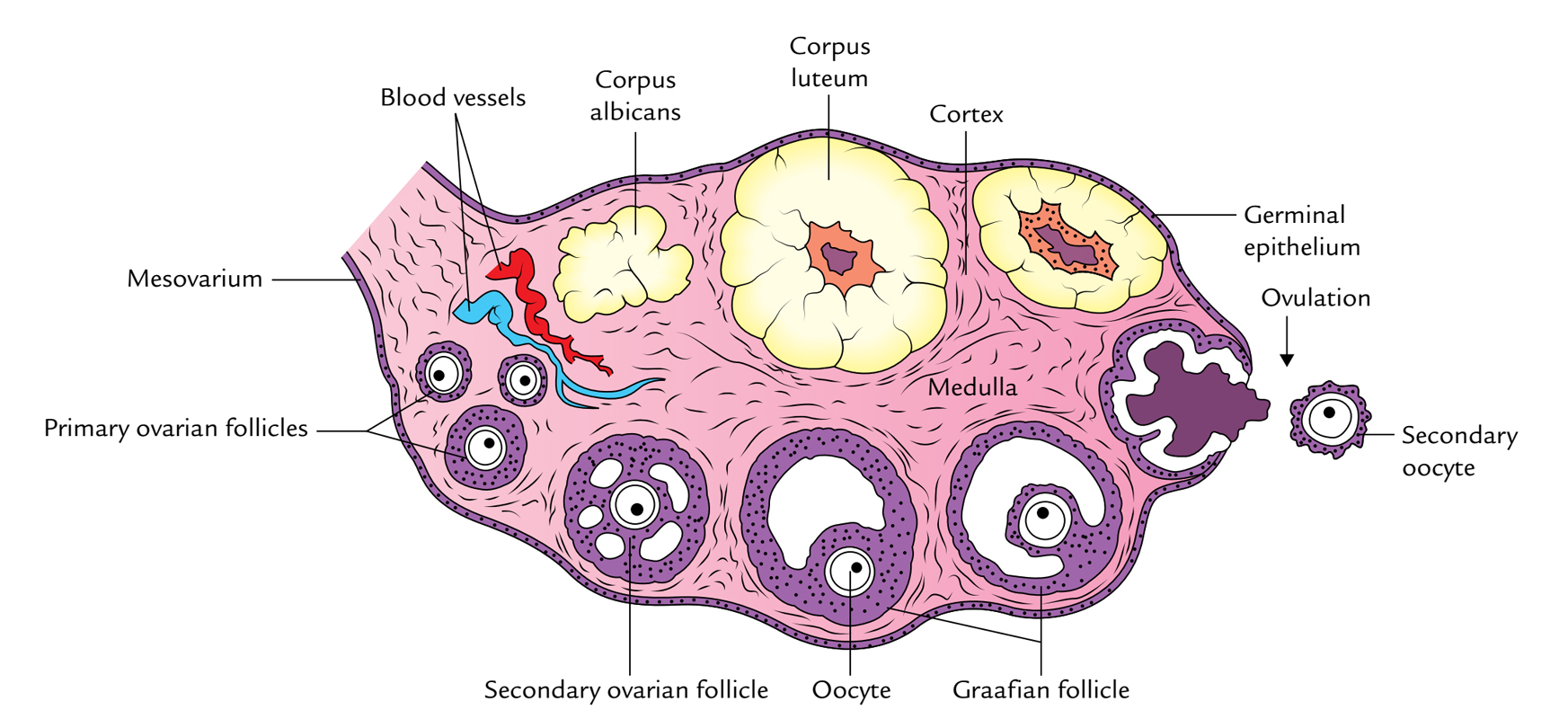
Ovaries are the primary source of estrogen and progesterone. These hormones influence breast growth, body shape, body hair, and regulate the menstrual cycle and pregnancy. During and after menopause, the ovaries stop releasing eggs and producing certain hormones.
Types of Ovarian Cancer
1. Epithelial Carcinoma
Epithelial carcinoma makes up 85% to 90% of ovarian cancers. The main types of epithelial tumors include serous, endometrioid, clear cell, mucinous, mixed tumors, and several rare malignancies, including Brenner tumors.
These types describe how these different ovarian/fallopian tube cancers are classified based on how they look under the microscope.
There can be differences in how these cancers behave and which treatments will work best. The vast majority of epithelial cancers are high-grade serous, meaning they resemble the cells lining the fallopian tube. These cancers are either high-grade serous cancers (HGSC) or low-grade serous carcinoma (LGSC).
High-grade serous cancers (HGSC) make up the vast majority of ovarian/fallopian tube cancer, most of which arise from the fallopian tube. Low-grade serous carcinoma (LGSC) is less common and may arise from the ovaries.
2. Germ Cell Malignancies
This uncommon type of ovarian cancer develops in the egg-producing cells of the ovaries. Germ cell malignancies typically occur in females 10 to 29 years old.
Types of germ cell tumors include dysgerminomas, immature teratoma, endodermal sinus tumors (called EST and yolk sac tumors), and embryonal carcinomas.
3. Sex Cord Stromal Tumors
This rare form of ovarian tumor develops in the connective tissue cells, called granulosa and theca cells, that hold the ovaries together. This tissue sometimes makes the female hormones estrogen and progesterone. Over 90% of these stromal tumors are called granulosa cell tumors, either adult or childhood types.
4. Granulosa Cell Tumors
Granulosa cell tumors may secrete estrogen, resulting in unusual vaginal bleeding at the time of diagnosis. Other types are Sertoli-Leydig cell tumors and steroid cell tumors.
Risk Factors of the Ovarian Cancer
A risk factor is anything that increases a person’s chance of developing cancer. Although risk factors often influence the development of cancer, most do not directly cause cancer.
Some people with several risk factors never develop cancer, while others with no known risk factors do. Knowing your risk factors and talking about them with your doctor may help you make more informed lifestyle and health care choices.
The following factors may raise a woman’s risk of developing ovarian cancer.
1. Family History
A strong family history of breast or ovarian cancer puts women at higher risk for ovarian cancer. Doctors believe this is because many of these families have genetic mutations, or changes in the gene, that are passed from generation to generation.
If you are concerned that ovarian cancer may run in your family, it is important to get an accurate family history, including any breast cancers in the family.
A family history of certain other types of cancer, including breast cancer, is linked to an increased risk of ovarian cancer. By understanding your family history, you and your doctor can talk about ways to reduce your risk and be proactive about your health.
2. Genetic Mutations
About 10% to 20% of ovarian cancers occur because a genetic mutation, or change, has been passed down within a family.
This inherited risk is called a germline mutation. American Society of Clinical Oncology (ASCO) recommends that all women diagnosed with epithelial carcinoma, the most common type of ovarian cancer, receive genetic testing at the time of diagnosis for several cancer risk genes, including BRCA1 and BRCA2, RAD51, and PALB.
This testing should be done regardless of whether there is a family history of ovarian or breast cancer. People who do not have an inherited genetic mutation should also be tested for BRCA mutations in the tumor cells, called somatic testing, as treatments for ovarian cancer with these mutations are effective regardless of whether the mutation is inherited.
A mutation in the BRCA1 or BRCA2 gene is associated with an increased risk of developing these cancers. A woman with an “average risk” has about a 1% to 2% lifetime risk of developing ovarian cancer.
A woman with a:
- BRCA1 mutation has around a 40% lifetime risk
- BRCA2 mutation has about a 10% to 20% lifetime risk.
BRCA-related ovarian cancers can occur in women who do not have a family history of either breast or ovarian cancer.
About 40% of women with ovarian cancer who are found to have a BRCA mutation do not have a family history. First-degree and second-degree family members should also receive genetic testing if a person with ovarian cancer has a BRCA mutation because the risk of these cancers can be inherited.
A genetic counselor can help you and/or your family members understand the results of genetic testing. The results of this testing can help determine your treatment options.
3. Genetic Conditions
Several rare genetic conditions cause ovarian cancer. Some of the most common include:
-
- Lynch syndrome. Lynch syndrome, also known as hereditary non-polyposis colorectal cancer, increases a woman’s risk of ovarian cancer and uterine cancer. It is caused by mutations in several different genes. Lynch syndrome also increases the risk of colorectal cancer and several other cancers.
- Peutz-Jeghers syndrome (PJS). PJS is caused by a specific genetic mutation. The syndrome is associated with multiple polyps in the digestive tract that become noncancerous tumors and with increased pigmentation (dark spots on the skin) on the face and hands. PJS raises the risk of ovarian cancer, breast cancer, colorectal cancer, cervical cancer, and several other types of cancer.
- Nevoid basal cell carcinoma syndrome (NBCCS). Women with NBCCS, also called Gorlin syndrome, have an increased risk of developing fibromas. Fibromas are benign fibrous tumors of the ovaries. There is a small risk that these fibromas could develop into a type of ovarian cancer called fibrosarcoma. People with NBCCS often have multiple basal cell skin cancers and jaw cysts and may develop medulloblastoma, a type of brain tumor, in childhood.
- Li-Fraumeni syndrome and ataxia-telangiectasia. Women with Li-Fraumeni syndrome or ataxia-telangiectasia may have a slightly increased risk of developing ovarian cancer.
- There may be other hereditary syndromes linked to these types of cancer, including small-cell carcinoma with an inherited SMARCA4 mutation and Sertoli-Leydig cell tumors with DICER1 syndrome. Research in this area is ongoing. Only genetic testing can determine whether a person has a genetic mutation. Most experts strongly recommend that people who are considering genetic testing first talk with a genetic counselor. This expert is specially trained and can explain the risks and benefits of genetic testing.
4. Age
A woman’s risk of developing ovarian cancer increases with age. Women of all ages have a risk of these cancers, but women over 50 are more likely to develop these cancers. About half of the women diagnosed with ovarian cancer are 63 years or older.
5. Obesity
Recent studies show that women who were obese in early adulthood, but not those who gain weight later in life, may have an increased risk of developing ovarian cancer. Women who are obese are more likely to die from any condition, including ovarian cancer.
6. Endometriosis
When the inside lining of a woman’s uterus grows outside of the uterus, affecting other nearby organs, it is called endometriosis.

This condition can cause several problems, but effective treatment is available. Researchers are continuing to study whether endometriosis is a risk factor for ovarian cancer. It may increase the risk of certain types of ovarian cancer, including clear cell and endometrioid ovarian cancers.
7. Ethnicities
Women of North American, Northern European, or Ashkenazi Jewish heritage have an increased risk of ovarian cancer. People of some of these ethnicities also have higher risks of BRCA mutations.
8. Reproductive History
Women may have an increased risk of ovarian cancer if they:
-
- Started their menstrual periods much earlier than the average age of about 12
- Have never given birth to a child
- Have unexplained infertility (the medical inability to have a child)
- Have not taken birth control pills
- Entered menopause much later than the average age of 51.
9. Hormone Replacement Therapy
Women who have taken estrogen-only hormone replacement therapy (HRT) after menopause may have a higher risk of ovarian cancer. The risk becomes higher the longer a woman uses the therapy. The risk decreases over time after the therapy ends.
Fertility drugs were once thought to increase the risk of ovarian cancer. It has been shown that they do not increase the risk.
Prevention of the Ovarian Cancer
Different factors cause different types of cancer. Researchers continue to look into what factors cause ovarian cancer, including ways to prevent it. Although there is no proven way to completely prevent ovarian cancer, you may be able to lower your risk.
Talk with your health care team for more information about your personal risk of cancer. Research has shown that certain factors may reduce a woman’s risk of developing ovarian cancer:
1. Taking Birth Control Pills
Women who took oral contraceptives for 3 or more years are 30% to 50% less likely to develop ovarian cancer. The decrease in risk may last for 30 years after a woman stops taking the pills. Intrauterine devices (IUDs) have also been linked to a decreased risk of ovarian cancer.
2. Breastfeeds
The longer a woman breastfeeds, the lower her risk of developing ovarian cancer.
3. Pregnancy
The more full-term pregnancies a woman has had, the lower her risk of ovarian cancer.
4. Surgical Procedures
Women who have had a hysterectomy or a tubal ligation may have a lower risk of developing ovarian cancer. A hysterectomy is the removal of the uterus and, sometimes, the cervix. Tubal ligation is having the fallopian tubes “tied” or closed surgically to prevent pregnancy.
Doctors recommend a bilateral salpingo-oophorectomy, which is the removal of both ovaries and fallopian tubes, for women with a high risk of ovarian cancer.
After a woman has given birth to all of the children she intends to have, she may choose to have her fallopian tubes removed at the time of abdominal surgery for other purposes or during a cesarean section, also called a c-section.
For women with high-risk genetic mutations such as BRCA1, BRCA2, and the genes related to Lynch syndrome, having the ovaries and fallopian tubes removed after having children is recommended to prevent ovarian cancers as well as possibly reduce the risk of breast cancer.
This can reduce ovarian cancer risk by as much as 96%. If performed before menopause occurs naturally, there may be a 40% to 70% reduction in the risk of developing breast cancer, particularly in women with BRCA2 mutations.
It is very important for women who are considering preventive surgery to talk with their doctors and genetic counselors so they can understand the risks and side effects of the surgery compared to their personal risk of developing ovarian cancer.
Symptoms and Signs of the Ovarian Cancer
Ovarian cancer can be hard to find in its earliest stages. That’s because the symptoms are often vague until these diseases are advanced. However, early-stage ovarian cancer versus advanced-stage ovarian cancer is not just a factor of delayed diagnosis but also of biology.
Most stage I ovarian cancers are clear cell, endometrioid, and mucinous with only a small percent being high-grade serous cancers (HGSC). The most advanced-stage ovarian cancers, however, are HGSC.
It is rare for women with ovarian cancer do not to have any symptoms. However, it’s also important to note that these symptoms are not specific to ovarian cancer and may be caused by a different medical condition that is not cancer. Often symptoms between early- and late-stage ovarian cancer will be similar.
Symptoms for ovarian cancer may include:
- Abdominal bloating
- Pelvic or abdominal pain
- Difficulty eating or feeling full quickly
- Urinary symptoms, such as urgency or frequency
- Fatigue
- Upset stomach
- Indigestion
- Back pain
- Pain with intercourse
- Constipation
- Menstrual irregularities
- Swelling in the pelvis or abdomen
- Vaginal discharge, which may be clear, white, or tinged with blood
For many women, these symptoms can be caused by reasons not related to ovarian cancer and can occur often. However, women need to acknowledge these symptoms if they begin and are different from what is normal for their bodies.
Women who have any of the symptoms listed above every day for more than a few weeks should see their primary care doctor or a gynecologist. A gynecologist is a doctor who specializes in treating diseases of the female reproductive organs.
Early medical evaluation may help find cancer at the earliest possible stage of the disease when it is easier to treat successfully.
Your doctor will ask how long and how often you’ve been experiencing the symptom(s), in addition to other questions. This is to help figure out the cause of the problem, called a diagnosis.
If the doctor diagnoses cancer, relieving symptoms remains an important part of cancer care and treatment. This may be called palliative care or supportive care. It is often started soon after diagnosis and is continued throughout treatment.
Be sure to talk with your health care team about the symptoms you experience, including any new symptoms or a change in symptoms.
Diagnosis of the Ovarian Cancer
Doctors use many tests to find or diagnose, cancer. They do tests to learn if cancer has spread to another part of the body from where it started. If this happens, it is called metastasis.
For example, imaging tests can show if cancer has spread. Imaging tests, such as ultrasound, computed tomography (CT) scan, or magnetic resonance imagining (MRI), show pictures of the inside of the body. Doctors may do tests to learn which treatments could work best.
If your primary care doctor suspects that you might have ovarian cancer, you should see a gynecologic oncologist. A gynecologic oncologist is a doctor who specializes in treating cancers of the female reproductive system.
Doing laboratory testing of the ovarian and fallopian tube tissues is the only sure way for the doctor to know if an area of the body has cancer. In most cases, this requires surgical removal of these organs.
This section describes options for diagnosing ovarian cancer. Not all tests listed below will be used for every person. Your doctor may consider these factors when choosing a diagnostic test:
- The type of cancer suspected
- Your signs and symptoms
- Your age and general health
- The results of earlier medical tests
While early detection and treatment are important, this is often not possible for ovarian cancer. There are no effective screening methods for ovarian cancer.
The reasons for this are because CA-125, which is tested using blood samples, can be at a higher level due to many benign conditions, especially endometriosis, fibroids, and pelvic inflammatory disease, in addition to pregnancy and menstruation.
Meanwhile, many benign conditions may look cancerous on transvaginal ultrasound. Large clinical trials have shown no benefit in screening the general population for ovarian cancer using these methods.
The annual Pap test that many women receive from their gynecologist does not check for ovarian cancer. It only identifies cervical cancer.
About 70% of epithelial ovarian cancers, particularly high-grade serous cancers, are not found until the disease is in an advanced stage and has spread to other parts of the body, most commonly the abdomen.
The following tests may be used to diagnose ovarian cancer:
1. Abdominal Pelvic Examination
Usually, the first exam is the abdominal-pelvic examination. The doctor feels the uterus, vagina, ovaries, bladder, and rectum to check for any unusual changes, such as a mass. Some cancers are very small before they spread and cannot be reliably felt and detected by pelvic examination.
A Pap test, usually done with a pelvic examination, is not likely to find or diagnose these cancers because that test is used to find cervical cancer.
2. Blood Tests / CA-125 Assay
There is a blood test that measures a substance called CA-125, which is a tumor marker. This marker is found in higher levels in women with ovarian cancer. Women younger than 50 with conditions such as endometriosis, pelvic inflammatory disease, and uterine fibroids may also have an increased CA-125 level.
This test is more accurate in women who have experienced menopause. Other tumor marker tests, such as HE4, are available, but none of these markers are effective for the early detection of these cancers.
3. Transvaginal Ultrasound
An ultrasound probe is inserted in the vagina and aimed at the ovaries and uterus. An ultrasound uses sound waves to create a picture of the ovaries, including surrounding tissues, cysts, and tumors. Researchers are studying whether this test can help with the early detection of ovarian cancer.
4. Computed Tomography (CT) Scan
A CT scan takes pictures of the inside of the body using x-rays taken from different angles. An x-ray is a way to create a picture of the structures inside the body using a small amount of radiation.
A computer combines these pictures into a 3-dimensional image that shows any abnormalities or tumors. Sometimes, a special dye called a contrast medium is given before the scan to provide better detail on the image.
This dye can be injected into a patient’s vein or given as a pill or liquid to swallow. A CT scan can be used to measure the tumor’s size and find out how much cancer has spread. While CT scan technology has continued to evolve, tumors or abnormalities smaller than about 5 millimeters (1/5th of an inch) are difficult to see.
5. Positron Emission Tomography (PET) or PET-CT Scan
A PET scan may be combined with a CT scan (see above), called a PET-CT scan. However, you may hear your doctor refer to this procedure as just a PET scan.

A PET scan is a way to create pictures of organs and tissues inside the body. A small amount of a radioactive sugar substance is injected into the patient’s body. This sugar substance is taken up by cells that use the most energy.
Because cancer tends to actively use energy, it absorbs more of the radioactive substance. A scanner detects this substance to produce images of the inside of the body. A PET-CT scan may only be used for certain people with ovarian cancer.
6. Magnetic Resonance Imaging (MRI)
An MRI uses magnetic fields, not x-rays, to produce detailed images of the body. MRI can be used to measure the tumor’s size. A special dye called a contrast medium is given before the scan to create a clearer picture. This dye can be injected into a patient’s vein.
7. Paracentesis
This is a medical procedure that removes peritoneal fluid that has built up in a person’s abdomen. This fluid buildup may be called ascites. A sample of the fluid is examined under a microscope for signs of cancer.
8. Biopsy
A biopsy is the removal of a small amount of tissue for examination under a microscope. Other tests can suggest that cancer is present, but only a biopsy can make a definitive diagnosis.
A pathologist analyzes the sample(s). A pathologist is a doctor who specializes in interpreting laboratory tests and evaluating cells, tissues, and organs to diagnose disease.
Biopsies for ovarian cancer are often done as part of the first surgery. During the surgery, doctors may remove as much of the tumor as possible. A tumor sample will be analyzed by a pathologist after the surgery is over.
A biopsy alone is sometimes used if the diagnosis is uncertain or if there is too much tumor to remove initially with surgery. This is usually done when chemotherapy is planned as the first treatment, with possible surgery afterward.
9. Molecular Testing of the Tumor
In addition to genetic testing for inherited, or germline, mutations, your doctor may also recommend running laboratory tests on a tumor to identify specific genes, proteins, and other factors unique to the tumor.
Genetic changes in the tumor cells are called somatic mutations. ASCO recommends that all women with epithelial ovarian cancer who do not carry a germline mutation receive somatic tumor testing.
Somatic tumor testing can look for BRCA1 and BRCA2 mutations in the tumor. And women with clear cell, endometrioid, mucinous, or other types of epithelial ovarian cancer should also be offered somatic testing for a feature called mismatch repair defect (dMMR).
This means the tumor does not repair damage to its DNA very well, which can lead the tumor to develop DNA mutations or changes. Results of these tests can help determine your treatment options.
After diagnostic tests are done, your doctor will review all of the results with you. As noted above, surgery and an examination of the lymph nodes may be needed before results are complete. If the diagnosis is cancer, these test results help the doctor describe cancer. This is called staging.
Statistics and Prognosis of the Ovarian Cancer
This year, an estimated 21,410 people in the United States will be diagnosed with ovarian cancer. The vast majority of these cases (90%) are high-grade serous ovarian cancers (HGSC), which begin in a fallopian tube.
From the mid-1980s to 2017, the number of new cases decreased by 1% to 2% each year. One reason for this decrease may be related to the decline in the use of hormone replacement therapy after a 2002 publication linked hormone replacement therapy to breast cancer risk, with later data showing an association with ovarian cancer.
The decrease may also be related to more women having their fallopian tubes removed. Ovarian cancer is more common in white women than in Black women.
Combined, cancer of the ovaries, fallopian tubes, and peritoneum are the fifth most common cause of cancer-related death in women in the United States. The death rate declined by around 2% each year from 2009 to 2018. This decline in the death rate is mostly due to advances in treatment.
The 5-year survival rate tells you what percent of people live at least 5 years after the cancer is found. Percent means how many out of 100.
The 5-year survival rate for people with all types of the ovarian, fallopian tube, and peritoneal cancers is 49%. However, the rate varies widely depending on the person’s age, as well as the stage, cell type, and grade of cancer.
Survival rates are also improved when debulking surgery is performed by a gynecologic oncologist instead of a gynecologist or general surgeon. The 5-year survival rate for women younger than 65 is 61%, compared with 32% for women age 65 and older.
If ovarian cancers are diagnosed and treated before they spread outside the ovaries and tubes, the general 5-year survival rate is 93%.
Approximately 16% of women with epithelial ovarian are diagnosed at this stage. If cancer has spread to surrounding tissues or organs, the 5-year survival rate is 75%. If cancer has spread to a distant part of the body, the 5-year survival rate is 30%. Approximately 58% of women are diagnosed at this stage.
It is important to remember that statistics on the survival rates for people with ovarian, fallopian tube, and peritoneal cancer are an estimate. The estimate comes from annual data based on the number of people with these cancers in the United States.
Also, experts measure the survival statistics every 5 years. So the estimate may not show the results of better diagnosis or treatment available for less than 5 years.