Treatment of Skin Cancer (Non-Melanoma)
Types of Treatment: Surgery, Sentinel Lymph Node Biopsy, Radiation Therapy, Chemotherapy, Targeted Therapy, Immunotherapy and Treatment options for Metastatic or Advanced Skin Cancer
Treatment of Skin Cancer (Non-Melanoma)
Different types of treatment are available for patients with non-melanoma skin cancer (basal cell carcinoma, squamous cell carcinoma of the skin), and actinic keratosis. Some treatments are standard, and some are being tested in clinical trials.
This section explains the types of treatments that are the standard of care for this type of cancer. “Standard of care” means the best treatments known (currently used for the treatment of skin cancer).
When making treatment plan decisions, you are encouraged to consider clinical trials as an option. A clinical trial is a research study that tests a new approach for the treatment of skin cancer. Doctors want to learn whether the new treatment is safe, effective, and possibly better than the standard treatment.
Clinical trials can test a new drug, a new combination of standard treatments, or new doses of standard drugs or other treatments. Clinical trials are an option to consider for treatment and care for all stages of cancer. Your doctor can help you consider all your treatment options.
Treatment overview
In cancer care, different types of doctors often work together to create a patient’s overall treatment plan that combines different types of treatments. This is called a multidisciplinary team. Cancer care teams include a variety of other health care professionals, such as physician assistants, nurses, social workers, pharmacists, counselors, dietitians, and others.
Descriptions of the common types of treatments used for basal cell carcinoma, squamous cell carcinoma, and Merkel cell cancer are listed below. Your care plan also includes treatment for symptoms and side effects, an important part of cancer care.
Treatment options and recommendations depend on several factors, including the size and location of the skin cancer, possible side effects, and the patient’s preferences and overall health. Take time to learn about all of your treatment options and be sure to ask questions about things that are unclear.
Talk with your doctor about the goals of each treatment and what you can expect while receiving the treatment. These types of talks are called “shared decision making.” Shared decision making is when you and your doctors work together to choose treatments that fit the goals of your care. Shared decision making is particularly important for non-melanoma skin cancer because there are different treatment options.
A. Surgery
Surgery is the removal of the tumor and surrounding tissue during a medical procedure. Many skin cancers can be removed from the skin quickly and easily during a simple surgical procedure. Often, no other treatment is needed.
Which surgical procedure is used depends on the type of skin cancer and the size and location of the lesion. Most of these procedures use a local anesthetic to numb the skin first.
They can be done by a dermatologist, surgical oncologist, general surgeon, plastic surgeon, nurse practitioner, or physician assistant in their clinic setting, outside of a hospital.
Others procedures, such as more extensive wide excisions and sentinel lymph node biopsies, are performed in a hospital operating room with local and/or general anesthesia. This is often done for Merkel cell cancer. Surgeries and other procedures for non-melanoma skin cancer include:
1. Curettage and Electrodessication
During this common procedure, the skin lesion is removed with a curette, which is a sharp, spoon-shaped instrument. The area is then treated with an electric current that helps control bleeding and destroys any remaining cancer cells. This is called electrodesiccation. Many people have a flat, pale scar after healing from this procedure.
2. Mohs Micrographic Surgery
This technique, also known as complete margin assessment surgery, involves removing the visible tumor in addition to small fragments around the edge of the area where the tumor was located.
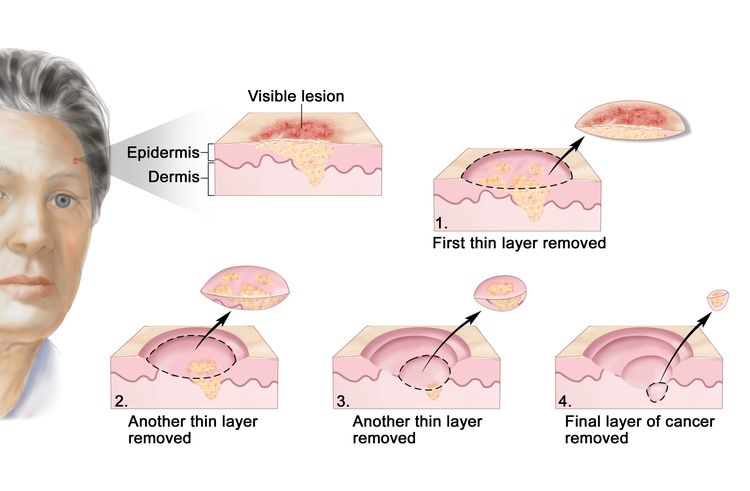
Each small fragment is examined under a microscope until all of the cancer is removed. This is typically used for larger tumors, for those located in the head-and-neck region, and for cancers that have come back in the same place.
3. Wide Excision
This involves the removal of the tumor and some surrounding healthy skin and soft tissue called a margin. How much tissue is removed depends on the type and size of the skin cancer.
When a large tumor is removed, the incision may be too large to close, so surgeons may use skin from another part of the body to close the wound. This is called a skin graft.
4. Reconstructive Surgery
Since skin cancer often develops on a person’s face, a reconstructive (plastic) surgeon or facial specialist may be part of the health care team. When doctors plan treatment, they consider how treatment might affect a person’s quality of life, such as how the person feels, looks, talks, and eats.
Before any surgery for skin cancer, talk with your doctor about whether changes to your appearance are possible and whether there may be functional aspects that need to be considered when developing a treatment plan.
5. Sentinel Lymph Node Biopsy
This surgical procedure also called sentinel lymph node biopsy (SLNB) or sentinel node biopsy (SNB), helps the doctor find out whether the cancer has spread to the lymph nodes. It is used for Merkel cell cancer. When cancer spreads from the place it started to the lymph nodes, it travels through the lymphatic system.
A sentinel lymph node is the first lymph node into which the lymphatic system drains. Because cancer can start anywhere on the skin, the location of the sentinel lymph nodes will be different for each patient, depending on where cancer started.
To find the sentinel lymph node, a dye, and a harmless radioactive substance are injected as close as possible to where the cancer started. The substance is followed to the sentinel lymph node. Then, the doctor removes 1 or more of these lymph nodes to check for cancer cells, leaving behind most of the other lymph nodes in that area.
These are sent to a pathologist who analyzes the lymph nodes and then provides a report. If cancer cells are not found in the sentinel lymph node(s), no further lymph node surgery is needed.
If the sentinel lymph node contains cancer cells, this is called a positive sentinel lymph node. This means the disease has spread, and the removal of more lymph nodes, called lymph node dissection, may be recommended.
Before surgery, talk with your health care team about the possible side effects from the specific surgery you will have. In general, surgery may include side effects such as pain, scarring, numbness, skin stretching, wound problems, infection, and changes in appearance where the surgery was performed.
B. Radiation Therapy
Radiation therapy is the use of high-energy rays or other particles to destroy cancer cells. A doctor who specializes in giving radiation therapy to treat cancer is called a radiation oncologist. Radiation therapy may be used instead of surgery for skin cancer that is located in a hard-to-treat place, such as on the eyelid, the tip of the nose, or the ear.
It is also used in some people who would like to avoid scarring from surgery. Sometimes radiation therapy may be recommended after surgery to help prevent the skin cancer from coming back.
For Merkel cell cancer, radiation therapy is often given after surgery for stage I and II disease. This is called adjuvant therapy.
The most common type of radiation treatment is called external-beam radiation therapy, which is radiation given from a machine outside the body. A radiation therapy regimen, or schedule, usually consists of a specific number of treatments given over a set period of time.
Several treatments may be needed to eliminate the cancer. A less common type of radiation treatment for skin cancer is brachytherapy. This involves placing the radiation source very close to or inside of the skin cancer.
Radiation therapy is not recommended for people with nevoid basal cell carcinoma syndrome.
The side effects from radiation therapy may include a rash, skin infections, itchy or red skin, or a change in the color of the skin. However, these side effects can usually be prevented by applying a corticosteroid or antibiotic to the skin. If side effects develop, most go away a few weeks after treatment has finished.
C. Other Local Treatments
To treat precancerous skin conditions or a cancerous lesion located only in the top layer of the skin, doctors may use photodynamic therapy, cryotherapy, or laser therapy.
1. Photodynamic Therapy
This is a combination treatment for actinic keratosis. First, a topical medication called aminolevulinic acid (Levulan) is applied over areas with many actinic keratoses. Then this area is exposed to a special light-emitting device for several minutes to a few hours.
The aminolevulinic acid makes the skin very sensitive, so the procedure can be painful. Your doctor may recommend taking pain medication before the procedure.
In addition, the chemical makes the skin very sensitive to the sun, so it is important to avoid sun exposure and wear protective glasses, clothing, and sunscreen for a few days after the procedure. The skin will remain very red and irritated for a few days, but the actinic keratoses quickly disappear once the redness goes away.
2. Freezing
This procedure, which is also called cryotherapy, uses liquid nitrogen to freeze and destroy abnormal cells. It is usually used to treat precancerous skin conditions.
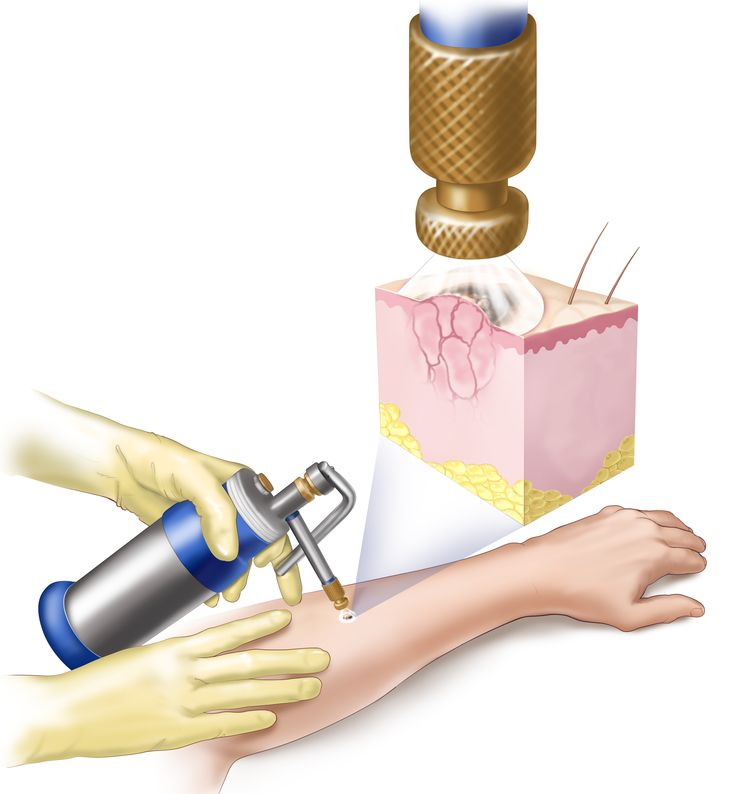
The liquid nitrogen will sting when it is first applied to the skin, and then the skin will blister and shed off. More than 1 freezing may be needed. Sometimes this procedure leaves a pale scar.
3. Laser Therapy
A narrow beam of high-intensity light can destroy precancerous skin conditions that are located only in the outer layer of the skin.
D. Therapies Using Medication
Systemic therapy is the use of medication to destroy cancer cells. This type of medication is given through the bloodstream to reach cancer cells throughout the body. Systemic therapies are generally prescribed by a medical oncologist, a doctor who specializes in treating cancer with medication.
Common ways to give systemic therapies include an intravenous (IV) tube placed into a vein using a needle or in a pill or capsule that is swallowed (orally).
The types of systemic therapies used for non-melanoma skin cancer include:
- Chemotherapy
- Targeted Therapy
- Immunotherapy
Each of these types of therapies is discussed below in more detail. A person may receive 1 type of systemic therapy at a time or a combination of systemic therapies given at the same time. They can also be given as part of a treatment plan that includes surgery and/or radiation therapy.
The medications used to treat cancer are continually being evaluated. Talking with your doctor is often the best way to learn about the medications prescribed for you, their purpose, and their potential side effects or interactions with other medications.
It is also important to let your doctor know if you are taking any other prescription or over-the-counter medications or supplements. Herbs, supplements, and other drugs can interact with cancer medications.
1. Chemotherapy
Chemotherapy is the use of drugs to destroy cancer cells, usually by keeping the cancer cells from growing, dividing, and making more cells.
In skin cancer treatment, these drugs are usually applied to the skin every day for several weeks. This is called topical treatment. These types of medications may cause skin inflammation or irritation, which will go away after treatment is finished.
Topical diclofenac (Solaraze), fluorouracil (Efudex), and ingenol mebutate (Picato) are approved for the treatment of precancerous actinic keratosis, with fluorouracil resulting in better results in terms of effectiveness and time until new precancers appear.
All of these creams can cause irritation, burning, redness, and stinging during treatment. These symptoms usually go away soon after treatment has been completed. These creams do not cause scars, which is why many doctors use them to treat the face or other areas where a person’s appearance may be affected.
For small basal cell cancers not located on the face, topical imiquimod (Aldara), which stimulates the immune system, may be recommended. The cream must be applied once a day, 5 days a week, for 6 to 12 weeks.
Topical fluorouracil is also approved by the U.S. Food and Drug Administration (FDA) to treat very thin basal cell carcinomas. It should be applied 2 times a day for 3 to 6 weeks. Some irritation and redness in the area of the basal cell carcinoma are expected with this treatment.
2. Targeted Therapy
Targeted therapy is a treatment that targets the cancer’s specific genes, proteins, or the tissue environment that contributes to cancer growth and survival. This type of treatment blocks the growth and spread of cancer cells while limiting damage to healthy cells.
For large (also called advanced) basal cell cancers that cannot be treated with surgery or radiation therapy, there are 2 targeted drugs, vismodegib (Erivedge) and sonidegib (Odomzo), which are FDA-approved drugs known as hedgehog pathway inhibitors.
They block the PTCH1 genetic mutation, which seems to drive the growth of basal cell carcinoma. This treatment shrinks or stabilizes tumors in many patients. The main side effects of this treatment include hair thinning, muscle cramps, weight loss, dry skin, and loss of taste.
Not all cancers have the same targets. To find the most effective treatment, your doctor may run tests to identify the genes, proteins, and other factors in your cancer cells. This helps doctors better match each patient with the most effective treatment whenever possible.
In addition, research studies continue to find out more about specific molecular targets and new treatments directed at them.
Talk with your doctor about the possible side effects of a specific medication and how they can be managed.
3. Immunotherapy
Immunotherapy also called biologic therapy, is designed to boost the body’s natural defenses to fight the cancer. It uses materials made either by the body or in a laboratory to improve, target, or restore immune system function.
An immune checkpoint inhibitor called cemiplimab (Libtayo) targets the PD-1 pathway. It is approved to treat metastatic or locally advanced squamous cell carcinoma and metastatic or locally advanced basal cell carcinoma.
The common side effects of cemiplimab include fatigue, rash, and diarrhea. It can also cause severe and possibly life-threatening side effects, including problems in the lung, intestines, liver, hormone gland, skin, and kidneys.
Pembrolizumab (Keytruda) is another immune checkpoint inhibitor that targets PD-1. The FDA has approved it for the treatment of Merkel cell cancer that has spread or come back after treatment.
Pembrolizumab is also approved to treat squamous cell carcinoma that has spread or come back after treatment and cannot be treated with surgery or radiation therapy. The common side effects of pembrolizumab include fatigue, pain, decreased appetite, itching, diarrhea, nausea, rash, fever, cough, shortness of breath, and constipation.
The FDA has also approved avelumab (Bavencio) to treat people 12 and older with Merkel cell cancer that has spread to another part of the body, called metastatic cancer. Avelumab blocks the PD-L1 pathway. By blocking this pathway, the body’s immune system may be able to more effectively fight cancer cells.
The common side effects of avelumab include fatigue, pain, diarrhea, nausea, rash, appetite loss, and swelling due to fluid buildup. Some patients also experience kidney problems, anemia, bowel obstruction, and infection.
Different types of immunotherapy can cause different side effects. Talk with your doctor about the possible side effects of the immunotherapy recommended for you.
E. Physical, Emotional, and Social Effects of Cancer
Cancer and its treatment cause physical symptoms and side effects, as well as emotional, social, and financial effects. Managing all of these effects is called palliative care or supportive care. It is an important part of your care that is included along with treatments intended to slow, stop, or eliminate the cancer.
Palliative care focuses on improving how you feel during treatment by managing symptoms and supporting patients and their families with other, non-medical needs. Any person, regardless of age or type, and stage of cancer, may receive this type of care.
And it often works best when it is started right after a cancer diagnosis. People who receive palliative care along with treatment for the cancer often have less severe symptoms, the better quality of life, and report they are more satisfied with treatment.
Palliative treatments vary widely and often include medication, nutritional changes, relaxation techniques, emotional and spiritual support, and other therapies. You may also receive palliative treatments similar to those meant to get rid of the cancer, such as chemotherapy, surgery, or radiation therapy.
Before treatment begins, talk with your doctor about the goals of each treatment in the treatment plan. You should also talk about the possible side effects of the specific treatment plan and palliative care options.
During treatment, your health care team may ask you to answer questions about your symptoms and side effects and to describe each problem.
Be sure to tell the health care team if you are experiencing a problem. This helps the health care team treat any symptoms and side effects as quickly as possible. It can also help prevent more serious problems in the future.
F. Metastatic or Advanced Skin Cancer
It is uncommon but non-melanoma skin cancer can spread to another part of the body from where it started. In these situations, doctors call it metastatic cancer.
If this happens, it is a good idea to talk with doctors who have experience in treating it. Doctors can have different opinions about the best standard treatment plan. Clinical trials might also be an option.
Surgery alone cannot always eliminate skin cancer that has metastasized. If cancer cannot be removed with surgery, it is called unresectable.
To control distant spread, a person’s treatment plan may include chemotherapy, radiation therapy, and/or targeted therapy. Palliative care will also be important to help relieve symptoms and side effects.
1. Squamous Cell Carcinoma
Metastatic or unresectable squamous cell carcinoma of the skin is rare, so treatment plans often use the same treatments that have worked in people with squamous cell carcinoma of the head and neck that may not have started on the skin.
Chemotherapy usually includes taxanes, such as docetaxel (Taxotere) or paclitaxel (Taxol), and platinums, such as carboplatin or cisplatin (both available as generic drugs).
The main side effects of these medicines include fatigue, low blood cell counts, rashes, diarrhea, and changes in sensation in the tips of the fingers or toes.
Targeted therapies may be used for some people with squamous cell carcinoma, including cetuximab (Erbitux), panitumumab (Vectibix), and erlotinib (Tarceva). These drugs are usually delivered through an intravenous (IV) tube placed into a vein using a needle or taken as tablets.
Recently, using immunotherapy to treat people with metastatic and unresectable squamous cell carcinoma has become more common. The PD-1 blocking drugs cemiplimab and pembrolizumab are approved for people with this diagnosis.
2. Basal Cell Carcinoma
If metastatic basal cell carcinoma cannot be treated with surgery or radiation therapy, targeted therapy may be an option. Vismodegib (Erivedge) and sonidegib (Odomzo) are FDA-approved drugs known as hedgehog pathway inhibitors.
They block the PTCH1 genetic mutation, which seems to drive the growth of basal cell carcinoma. This treatment shrinks tumors in many patients. The main side effects of this treatment include hair thinning, muscle cramps, weight loss, dry skin, and loss of taste.
3. Merkel Cell Cancer
Treatment for metastatic Merkel cell cancer usually involves immunotherapy with avelumab or pembrolizumab (see “Immunotherapy,” above). Other immunotherapy medications may be available through clinical trials. Chemotherapy, surgery, and/or radiation therapy may be used to relieve symptoms and side effects.
For most people, a diagnosis of metastatic cancer is very stressful and, at times, difficult to bear. You and your family are encouraged to talk about how you feel with doctors, nurses, social workers, or other members of the health care team. It may also be helpful to talk with other patients, including through a support group.
G. Remission and Chance of Recurrence
A remission is when cancer cannot be detected in the body and there are no symptoms. This may also be called having “no evidence of disease” or NED.
A remission may be temporary or permanent. This uncertainty causes many people to worry that the cancer will come back. While many remissions are permanent, it is important to talk with your doctor about the possibility of the cancer returning. Understanding your risk of recurrence and the treatment options may help you feel more prepared if the cancer does return.
If skin cancer returns after the original treatment, it is called recurrent cancer. It may come back in the same place (called a local recurrence), nearby (regional recurrence), or in another place (distant recurrence). Certain parts of the body, such as the ears and lips, are more prone to develop recurrent skin cancers.
In addition, people whose immune system is suppressed due to a medication or disease are also at higher risk for skin cancer recurrence.
When this occurs, a new cycle of testing will begin again to learn as much as possible about the recurrence. After this testing is done, you and your doctor will talk about the treatment options. Often the treatment plan will include the treatments described above.
Your doctor may suggest clinical trials that are studying new ways to treat this type of recurrent cancer. Whichever treatment plan you choose, palliative care will be important for relieving symptoms and side effects.
People with recurrent cancer often experience emotions such as fear. You are encouraged to talk with the health care team about these feelings and ask about support services to help you cope.