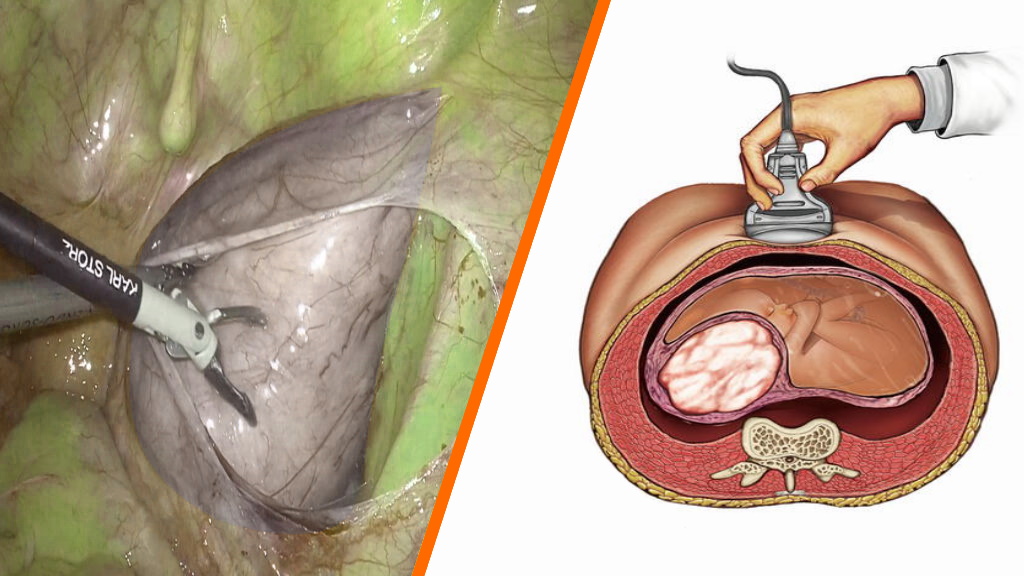
Laparoscopic Retroperitoneal Parasitic Myoma Excision
Wandering or Migrating Myoma
Parasitic Myomas
The conventional thinking is that parasitic myomas are a rare variant of pedunculated subserosal myomas. It has been suggested that if a pedunculated subserosal myoma develops a long stalk and becomes what is termed a “wandering, migrating or parasitic myoma” such a tumor can then go on to adhere to surrounding structures such as the omentum or broad ligament and develop an auxiliary blood supply. In this way, a “parasitic myoma” is formed when a “wandering myoma” loses its uterine blood supply and becomes attached and fed from a nonuterine source. Occasionally a broad ligament leiomyoma is also classified under parasitic myomas.
Uterine myomas occur in approximately 25% of reproductive-aged women and are noted on pathologic examination in approximately 80% of surgically excised uterus.
The subset of parasitic myomas is rare, with few reported cases in the literature. Although first described by Kelly and Cullen in 1909, as “myomata that have for some reason become partially or almost completely separated from the uterus and receive their main blood-supply from another source,” the cause, natural history, and pathologic basis of parasitic myomas are still not clearly understood.
The literature has been limited to case reports and small series of such findings since the early 1900s; more recently, a few case studies have identified parasitic myomas after laparoscopic morcellation procedures.
Diagnosis of parasitic myomas is often incidental at the time of abdominal surgery for treatment of symptoms due to uterine myomas; however, there are case reports in which parasitic myomas have been found to cause symptoms themselves.
Radiographic Features
On imaging, parasitic myomas present as solid pelvic or abdominal masses with characteristics similar to uterine myomas.
Treatment and Prognosis
With behavior similar to uterine myomas, parasitic myomas may recur after resection or, conversely, may show hormone-responsive behavior, including size stability or even shrinkage with natural, surgical, or chemical menopause.
Surgery is usually performed for symptomatic relief or to prevent impingement of vital structures.
Differential Diagnosis
The differential diagnosis for parasitic myomas varies with their locations can include:
- Ovarian Stromal Tumors
- Leiomyosarcoma
- Drop Metastases
- Lymphadenopathy
Primary References
-
A parasitic myoma – International Journal of Reproduction …
-
Parasitic myomas. Kimberly A Kho , Ceana Nezhat. Obstet Gynecol, 2009 Sep;114(3):611-5.