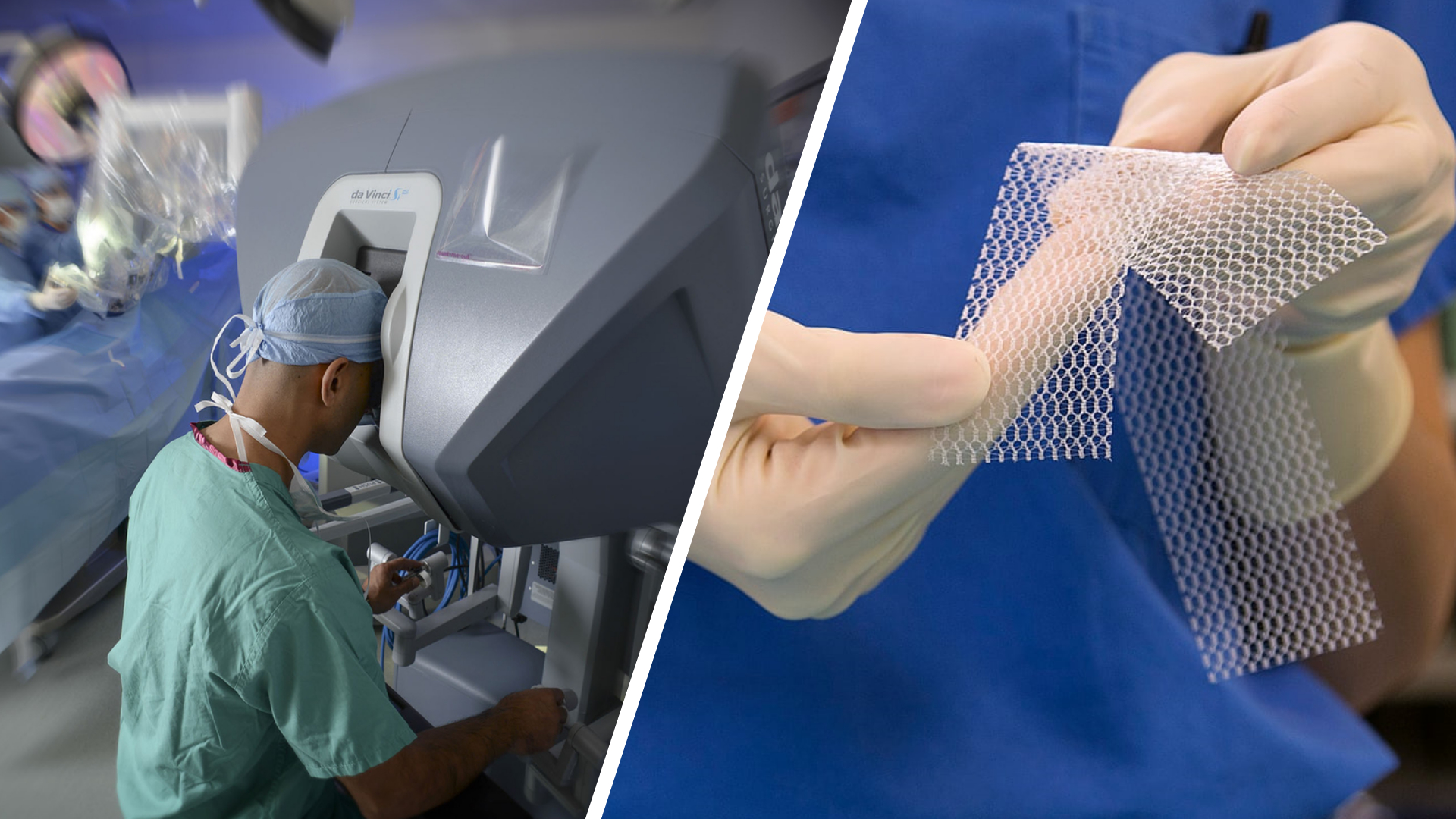
Robotic Ventral Hernia Repair with Mesh Placement
In the past decade, the use of robotic platforms in surgery has grown exponentially, reaching a fourfold increase in the number of procedures performed worldwide with robotic assistance from 200 000 in 2009 to nearly 900 000 procedures a year in 2017.
General surgery has seen the fastest growth of all surgical specialties, and hernia repairs are among the most commonly performed general surgery procedures. This growth occurred despite limited evidence supporting the practice of robotic ventral hernia repair (RVHR).
The concept of hernias and their treatment have been present since the beginning of human history. Treatment of hernias has progressed alongside the development of surgery, and the evolution of hernia repair has been facilitated by new prosthesis technology.
The fascination with hernia surgery is in part driven by its prevalence and by the variety of treatment options.
Herniorrhaphy, however, is not without its risks of complications. The goal of hernia surgery is for a robust repair while minimizing complications.
Minimally invasive hernia surgery treats the problem with less risk for common complications encountered with open surgery.
New techniques in minimally invasive hernia surgery are arising from previous open methods, and more complex abdominal wall hernias are now approached robotically.
These results are promising for patients with complex abdominal hernias who may require a strong anatomic repair but who can still benefit from a minimally invasive approach.
An abdominal wall hernia is defined as the protrusion of intra-abdominal tissue through a defect in the abdominal wall, known as ventral hernia.
Hernias can be either the enlargement of a natural anatomic defect (hiatal or inguinal hernias) or the development of a new defect in a compromised tissue. The ventral hernia category includes umbilical, epigastric, and spigelian hernias.
Recently, a retrospective national database study published by the Americas Hernia Society Quality Collaborative compared the most commonly performed minimally invasive ventral hernia repair techniques: robotic ventral hernia repair (RVHR) with intraperitoneal onlay mesh placement and laparoscopic ventral hernia repair (LVHR) with intraperitoneal onlay mesh placement.
This study showed a shorter postoperative hospital length of stay with robotic ventral hernia repair (RVHR) (0 days in the robotic ventral hernia repair (RVHR) group versus 1 day in the laparoscopic ventral hernia repair (LVHR) group; P≤0.001) and no differences in safety or clinical outcomes.
Robotic Ventral Hernia Repair (RVHR)
Ventral hernia repairs were performed using conventional approaches recommended by surgical societies.
Common steps of both procedures were as follows:
1. The abdomen was entered in the right or left upper abdominal quadrant with an optical trocar; a pneumoperitoneum was created by insufflating the abdomen with CO2 to an intra-abdominal pressure of 10~15 mm Hg.
2. RVHR was performed using three 8-12 mm ports placed along the lateral abdomen, the robotic platform was docked, all adhesions were taken down with robotic scissors and grasper, the fascial defect was closed with 0 locking barbed polydioxanone suture;
3. A mid-density hydrogel adhesion barrier coated polypropylene mesh was used; mesh size was selected to provide at least 5 cm of overlap on all sides relative to the hernia defect and was then secured to the anterior abdominal wall through an intraperitoneal onlay mesh placement technique;
4. The mesh was secured intraperitoneally with circumferential running 2-0 barbed polydioxanone suture, and all 12 mm ports were closed with 0-polyglactin suture.
During robotic intraperitoneal onlay mesh placement repair, the mesh is commonly fixated using a running suture. Alternatively, for laparoscopic repair, four cardinal sutures are commonly used, along with tacks in a single or double crown.
New innovations can be disruptive in both a positive and a negative fashion. For example, an era of smaller incisions, fewer incisional hernias, improved quality of life for patients, shorter length of stay in hospital, improved recovery, and improved return to work came with the introduction of minimally invasive endoscopic techniques.
However, during its early adoption, laparoscopic and robotic surgeries also resulted in more major complications such as enterotomies, bile duct injuries, and major vascular injuries. With time, as the technology improves, robotics may and will probably be the future of surgery in the long term.
Primary References:
- Current perspectives in robotic hernia repair. Robot Surg. 2017 May 5;4:57-67.
- Robotic-Assisted Transabdominal Preperitoneal Ventral Hernia Repair. Surg Technol Int. 2020 May 28;36:95-97.